
In a remarkable testament to medical ingenuity, a critical patient has been successfully kept alive for two full days without the function of his own lungs, a period during which his life was entirely supported by an extracorporeal artificial lung system, awaiting a life-saving double lung transplant. This groundbreaking clinical case, detailed in a recent publication in the scientific journal Med by Cell Press, offers compelling evidence for a novel therapeutic strategy: utilizing advanced mechanical support to bridge the gap for individuals suffering from overwhelming lung damage, thereby creating a crucial window for organ transplantation when conventional treatments prove insufficient.
The individual at the center of this medical drama, a 33-year-old man, presented with a catastrophic cascade of organ failure, a dire consequence of a severe, rapidly progressing infection. His initial affliction, a seemingly common influenza infection, tragically evolved into a virulent bacterial pneumonia, triggering a devastating inflammatory response known as acute respiratory distress syndrome (ARDS). This severe form of lung injury, characterized by widespread inflammation and fluid accumulation within the lung alveoli, progressively crippled his respiratory capacity. As his lungs deteriorated to a point where they were described as "melting" and irrecoverably compromised, his vital organs, including his heart and kidneys, began to falter, pushing him to the brink of death. The situation was so critical that upon arrival at the hospital, his heart had ceased functioning, necessitating immediate cardiopulmonary resuscitation.
The severity of the infection had rendered the patient’s native lungs beyond any hope of recovery. More critically, these damaged organs were actively contributing to the systemic spread of the infection, creating a dangerous feedback loop that threatened his survival. However, the patient’s physiological state was too fragile and unstable to undergo the immediate, complex procedure of a double lung transplant. This created a critical dilemma for the medical team: how to maintain adequate oxygenation and carbon dioxide removal for the body when the primary organs responsible for these functions were failing and had to be surgically removed to combat the infection.
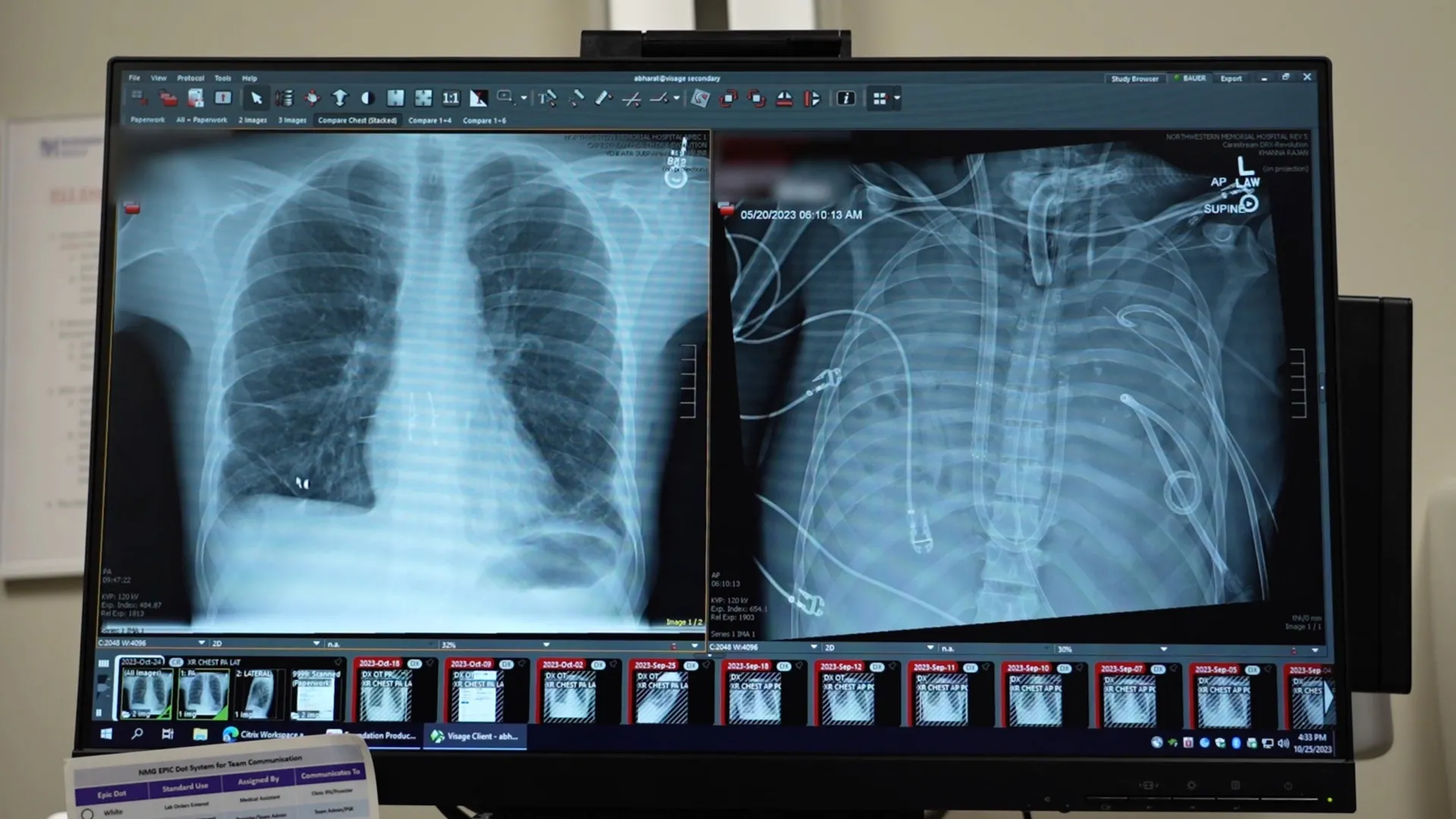
Addressing this unprecedented challenge, the surgical team at Northwestern University, led by thoracic surgeon Ankit Bharat, devised and implemented a sophisticated extracorporeal membrane oxygenation (ECMO) system, specifically configured to function as an "artificial lung." This advanced technology was meticulously engineered to replicate the essential functions of healthy lungs. Blood was drawn from the patient’s body, circulated through the artificial lung where it was infused with oxygen and cleansed of carbon dioxide, and then returned to the bloodstream, effectively bypassing the diseased pulmonary system. This critical intervention provided the necessary physiological support, allowing the patient’s heart and other organs to stabilize and begin a process of recovery, even in the complete absence of native lung function.
Following the surgical removal of his severely infected lungs, the patient’s condition began to show marked improvement. His circulatory system stabilized, his blood pressure normalized, and the overwhelming infection started to recede, bringing the rampant spread of pathogens under control. This period of stabilization, made possible by the artificial lung system, was instrumental in preparing him for the definitive treatment. After a tense 48-hour waiting period, compatible donor lungs became available, and a complex, multi-hour double lung transplant surgery was successfully performed. Remarkably, more than two years post-transplant, the patient has recovered fully and is now living a normal, active life with robust lung function, a profound testament to the efficacy of this integrated approach.
This case challenges conventional medical thinking regarding the management of severe ARDS. Traditionally, lung transplantation has been primarily reserved for patients with chronic, progressive lung diseases such as interstitial lung disease or cystic fibrosis. The prevailing assumption for acute respiratory failure, including severe ARDS, has often been that supportive care and time would allow the lungs to heal and recover. However, a detailed molecular examination of the patient’s explanted lungs revealed extensive and irreversible scarring, coupled with significant immune system damage. These pathological findings provided definitive biological evidence that, in certain extreme cases of ARDS, the lung tissue is fundamentally incapable of regeneration, rendering transplant the only viable curative option.
The findings from this case offer crucial molecular validation for the necessity of lung transplantation in specific patient populations suffering from acute, overwhelming lung injury, a reality previously inferred but not biologically proven. It underscores that for a subset of patients experiencing ARDS, especially those with rapidly progressive and destructive lung damage stemming from infections or other acute insults, maintaining them with conventional ventilation is insufficient, and transplantation may be the only pathway to survival.
While the approach employed in this case is currently resource-intensive and requires highly specialized expertise, facilities, and a dedicated multidisciplinary team, it holds immense promise for the future of critical care medicine. Dr. Bharat expressed optimism that this methodology could evolve into more standardized and accessible protocols, thereby expanding the potential for lung transplantation to serve as a critical "bridge" for a broader range of critically ill patients awaiting donor organs. He noted that tragically, young patients with severe, acute lung damage often succumb to their conditions because the possibility of a lung transplant as an emergency intervention is not recognized or considered early enough. This pioneering case suggests that for acute lung failure induced by severe infections or viral illnesses, even in emergency settings, a lung transplant should be a more readily considered life-saving option. The successful application of the artificial lung system in this instance not only saved a life but also significantly advanced our understanding of acute lung injury and the potential of extracorporeal support in organ transplantation.
About the Author










{kind=link}