
In a groundbreaking medical feat, a patient was kept alive for a full 48 hours without functioning lungs, a period during which their native organs were surgically removed and replaced with a sophisticated extracorporeal membrane oxygenation (ECMO) system, effectively acting as an artificial lung, until a life-saving double lung transplant could be successfully performed. This remarkable case, meticulously documented and published in the prestigious journal Med by Cell Press, offers a compelling glimpse into a novel strategy for sustaining critically ill individuals awaiting vital organ donations, challenging previous assumptions about the absolute necessity of native lung function for survival in acute respiratory failure scenarios.
The patient, a 33-year-old male, presented with an alarmingly severe presentation of acute respiratory distress syndrome (ARDS), a life-threatening condition characterized by widespread inflammation and infection within the lungs, leading to profound respiratory compromise. His initial illness stemmed from a severe influenza infection, which rapidly deteriorated and became complicated by a secondary bacterial pneumonia. As his condition spiraled, his respiratory system, along with his cardiac and renal functions, began to fail catastrophically. At this critical juncture, a double lung transplant emerged as his sole viable option for survival, a procedure complicated by the extreme instability of his overall health.
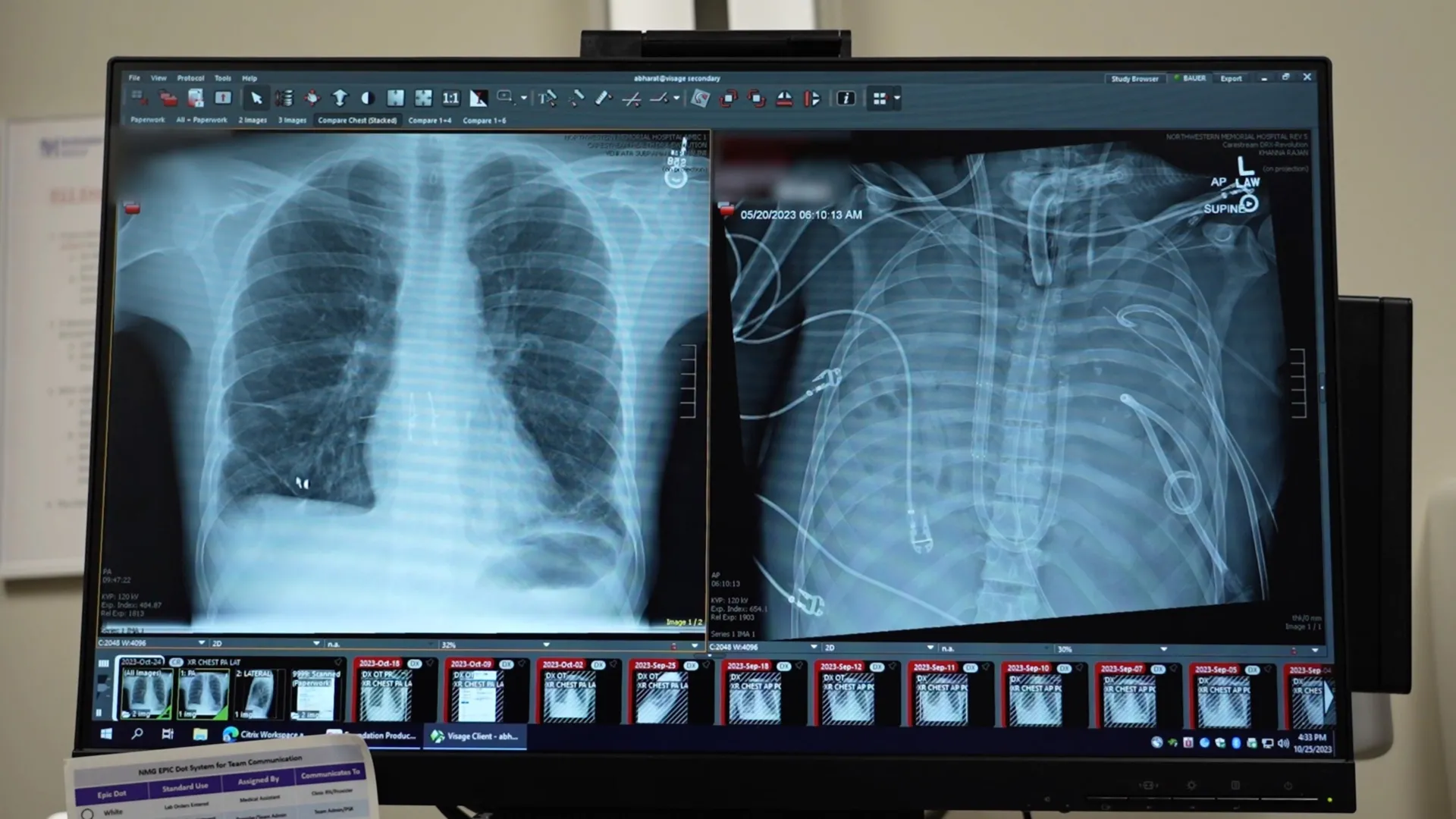
The urgency of the situation was underscored by the patient’s arrival, during which his heart had stopped, necessitating immediate cardiopulmonary resuscitation (CPR). Lead author Ankit Bharat, a thoracic surgeon at Northwestern University, described the dire circumstances, explaining that when lung tissue becomes so ravaged by infection that it effectively "melts," the damage is irreversible, and survival is typically impossible. In this particular case, the severely infected lungs were not only non-functional but were actively propagating the infection throughout the patient’s body, posing an immediate and overwhelming threat. However, the patient’s precarious physiological state rendered him too unstable for an immediate transplant, creating a critical window where medical intervention was needed to stabilize him before the complex surgical procedure could be attempted.
The intricate connection between the heart and lungs presented a significant challenge: how to maintain circulation and oxygenation in the absence of the primary respiratory organs. To bridge this gap, the dedicated medical team devised and implemented an innovative artificial lung system. This ECMO configuration was meticulously engineered to assume the vital functions of the patient’s lungs. It expertly oxygenated the circulating blood, efficiently removed carbon dioxide, and provided crucial circulatory support, thereby enabling the patient’s heart and other vital organs to continue functioning adequately despite the complete absence of his native lungs.
Following the surgical removal of his critically diseased lungs, the patient’s clinical status began to show signs of stabilization and improvement. His blood pressure normalized, his failing organs started to recover, and the rampant infection was gradually brought under control. This period of critical stabilization, facilitated by the artificial lung, lasted for two days, during which time a suitable donor organ became available. Surgeons then proceeded with the complex double lung transplant, which was performed successfully. More than two years post-transplantation, the patient has made a full recovery and is living a normal life, demonstrating the profound efficacy of this integrated approach to critical care.
This case also offers compelling new insights into the nature of irreversible lung damage, particularly in the context of severe ARDS. Traditionally, lung transplantation has been predominantly reserved for patients suffering from chronic, degenerative lung conditions such as interstitial lung disease or cystic fibrosis. The prevailing medical consensus has often held that in cases of severe ARDS, supportive care aimed at helping the lungs recover over time is the primary strategy. However, a detailed molecular analysis of the patient’s explanted lungs revealed extensive and irreparable scarring, alongside significant immune system damage, providing irrefutable biological evidence that this specific tissue was beyond any possibility of recovery.
Dr. Bharat emphasized the significance of these findings, stating that this case provides, for the first time, biological and molecular validation that certain patients with severe lung damage due to ARDS will unequivocally require a double lung transplant to survive. Without such intervention, their prognosis is grim.
While this advanced technique is currently confined to highly specialized medical centers equipped with the necessary expertise, infrastructure, and resources, Dr. Bharat expresses optimism that it can evolve into more standardized and accessible systems. The ultimate goal is to provide a reliable "bridge to transplant" for patients facing life-threatening respiratory failure, ensuring they can survive the critical waiting period for donor organs. Dr. Bharat noted a deeply concerning reality in his own practice: the weekly loss of young patients who might have been saved if transplantation had been considered an earlier or more viable option for acute lung damage caused by viral infections or other severe inflammatory processes. This revolutionary application of ECMO and the subsequent successful transplant underscore the potential for lung transplantation to be a life-saving intervention even in acute settings, challenging established paradigms and offering renewed hope to patients facing the most severe forms of respiratory failure.
About the Author







{kind=link}