
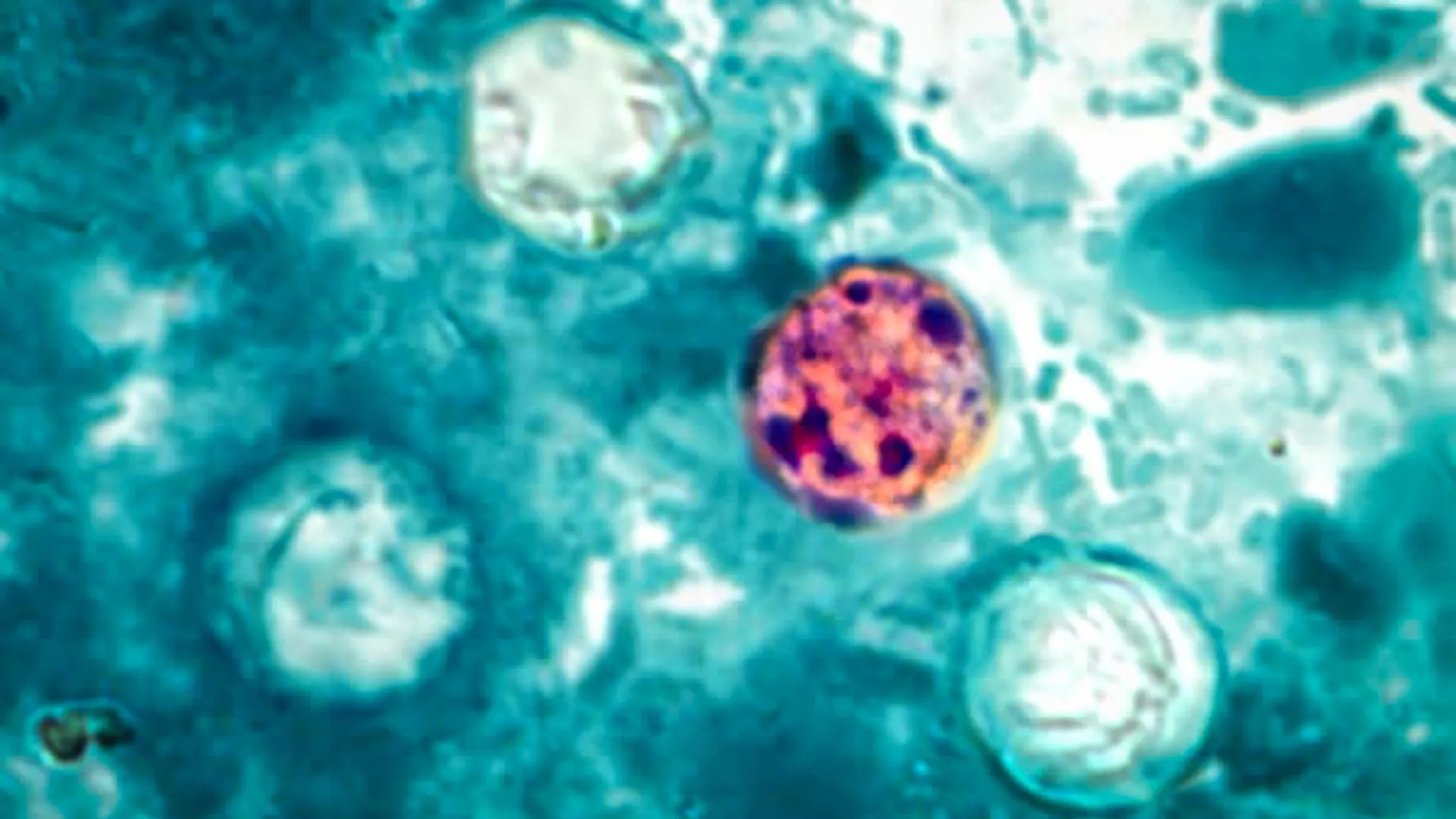
The U.S. Centers for Disease Control and Prevention (CDC), in conjunction with a consortium of state and federal health departments, is actively engaged in a comprehensive investigation into a series of escalating cyclosporiasis outbreaks that have impacted communities across the United States. The primary objective of this collaborative effort is to pinpoint and definitively identify the origin of the parasitic infections, a task that remains ongoing as data continues to be meticulously collected and analyzed.
A significant cluster of cyclosporiasis cases has emerged, prominently affecting at least four states within the Midwestern region, prompting intensive public health scrutiny. Health officials are employing a crucial investigative technique: conducting detailed interviews with individuals who have fallen ill. These conversations are designed to meticulously reconstruct dietary histories, focusing on the foods consumed in the period preceding the onset of their symptoms. This approach aims to identify any commonalities in food consumption that might link the affected individuals to a shared source of contamination.
Despite the rigorous efforts underway, a definitive food product implicated as the sole source of this widespread contamination has not yet been officially confirmed. Public health authorities are diligently accumulating and processing a vast amount of information, meticulously sifting through every available data point in their pursuit of identifying the etiological agent responsible for the current outbreak. This investigative process is complex, often requiring the analysis of intricate supply chains and consumption patterns.
Concerns within the public health sector have been amplified by a discernible uptick in cyclosporiasis diagnoses beginning in early May. Beyond the substantial outbreak concentrated in the Midwest, federal and state health agencies are simultaneously examining several other localized clusters of illness that have surfaced in various parts of the country. This suggests that the problem may be more diffuse than initially understood, potentially involving multiple independent contamination events or a single, far-reaching source affecting different geographic areas.
Cyclosporiasis, while not typically a life-threatening condition for the majority of those infected, can, in some instances, lead to severe illness necessitating hospitalization. The parasitic infection can cause debilitating gastrointestinal distress, and prompt medical attention is strongly advised for anyone experiencing symptoms consistent with the illness. Early diagnosis and appropriate treatment can significantly mitigate the severity and duration of the condition.
The investigation involves a multifaceted data collection strategy, with the CDC, state-level public health and regulatory bodies, and the U.S. Food and Drug Administration (FDA) all contributing to the review of diverse information streams. This collaborative approach ensures that all angles are explored, from agricultural practices and food processing to distribution networks and consumer purchasing habits. The sheer volume of data requires sophisticated analytical tools and significant inter-agency coordination.
As of July 13th, reports submitted to the CDC indicated that over 400 individuals have been identified as infected with Cyclospora in connection with the current outbreak. The geographical distribution of these confirmed cases is currently concentrated in Michigan, Ohio, West Virginia, and Kentucky, highlighting the regional nature of this particular surge. However, the possibility of cases existing outside these confirmed states is a significant area of ongoing inquiry.
The CDC has also acknowledged the existence of additional reported illnesses that are still undergoing thorough investigation to ascertain their definitive link to the ongoing outbreak. Individuals reporting illness associated with this outbreak have indicated a sickness onset on or after June 22, 2026. This temporal clustering is a critical piece of information for epidemiological tracing.
Health officials operate under the informed assumption that the actual number of infections likely surpasses the officially documented figures. Several factors contribute to this discrepancy. Many individuals who contract cyclosporiasis may experience mild symptoms and recover without seeking formal medical care, thereby never being tested and officially counted. Furthermore, there is an inherent lag time in the diagnostic process; it can take several weeks for a newly diagnosed case to be definitively linked to a broader outbreak, meaning recent illnesses may not yet be reflected in the reported totals. This delay underscores the dynamic nature of outbreak investigations.
To facilitate the identification of the contaminated food source, public health investigators systematically gather comprehensive demographic data from affected patients. This includes information pertaining to their age, race, ethnicity, and other relevant demographic identifiers. Crucially, detailed accounts of their dietary intake during the incubation period are collected. The analysis of these responses is designed to uncover potential patterns and correlations that can guide investigators in tracing the contamination back to its origin within the food supply chain. This painstaking process of data aggregation and pattern recognition is central to solving foodborne illness outbreaks.
Individuals experiencing symptoms suggestive of cyclosporiasis are strongly urged to seek prompt consultation with a healthcare professional. The onset of symptoms can vary, typically appearing approximately one week after exposure to the parasite, with the incubation period ranging from as little as two days to as long as two weeks or even more. Without timely and effective treatment, the symptoms, which primarily manifest as gastrointestinal distress including diarrhea, loss of appetite, abdominal cramping, bloating, and nausea, can persist for an extended duration, potentially lasting for several days, a month, or even longer, significantly impacting an individual’s quality of life.
The cooperation of diagnosed individuals is vital in assisting public health investigators in their pursuit of the contaminated food item. Local and state health departments may reach out to those confirmed to have cyclosporiasis, requesting detailed information about their food consumption in the two weeks preceding their illness. Providing accurate and thorough details about meals, ingredients, and where food was purchased or consumed can significantly accelerate the identification of the specific food product responsible for the outbreak, thereby enabling the implementation of targeted control measures.
To mitigate the risk of cyclosporiasis infection, consumers are advised to stay informed about foods that have historically been associated with outbreaks of this parasitic illness and to familiarize themselves with preventive measures recommended by health authorities. Adherence to proper food handling and preparation techniques, along with thorough washing of produce, are fundamental steps in reducing exposure. Staying abreast of current food recalls and ongoing outbreak investigations through official channels, such as the CDC’s food safety alerts, is also a crucial component of personal and public health vigilance.
Healthcare providers play a critical role in the early detection and reporting of cyclosporiasis cases. They are encouraged to promptly report any diagnosed instances of the illness to their local health department. This immediate notification is essential for initiating timely public health responses and for accurately tracking the scope of the outbreak. Comprehensive clinical guidance, including detailed information on symptoms, diagnostic approaches, treatment protocols, and patient management strategies for cyclosporiasis, is readily available through resources such as the CDC’s Clinical Care of Cyclosporiasis guidelines, empowering healthcare professionals to provide optimal care and contribute effectively to outbreak control efforts.
About the Author









{kind=link}